
Discuss this article on the forums
Thanks to Lannie for allowing us to publish her overview (complete with slide!) of the Jan 17th from talk by Dr. Mikovits and Annette Whittemore. (headings added) Find the original here

PART 1: 1/17/11 XMRV presentation by Dr. Judy Mikovits and Annette Whittemore
Today I attended “Chronic Fatigue Syndrome, the XMRV Retrovirus, and the Human MLV-related Viruses: The latest on testing, treatments and research into XMRV and its relationship to chronic inflammatory neuroimmune disease, including Chronic Fatigue Syndrome, Multiple Sclerosis, Fibromyalgia, Chronic Lyme Disease and Cancer” organized and hosted by Gordon Medical Associates in Santa Rosa, CA. Presenters were Dr. Judy Mikovits, Director of Research, Whittemore Peterson Institute and Annette Whittemore, President and Founder, Whittemore Peterson Institute.
I would be curious about the final headcount, but if I had to estimate I’d guess approximately 150 people were in attendance. Gordon Medical Associates did a fantastic job organizing the event. It started off a little shaky as Dr. Mikovits was stuck on a plane en route from Reno. However, highlighting the collaborative nature of the WPI, Annette Whittemore took to the stage and presented a large part of Judy’s presentation eloquently and thoroughly – saving only the scientific diagrams for when Dr. Mikovits arrived.
_______________________________________
Genesis of an Institute – The presentation started with a bit of background on the Whittemore Peterson Institute (WPI), including the building itself. The building came to be simply out of the need for visibility and collaboration. Whittemore knew the disease ailing her daughter was multi-systemed, and there were many different types of specialists required to address the research needs of CFS. She saw many of these different types of specialists were housed in buildings throughout the University of Nevada-Reno. Instinctively she knew the only way to effectively collaborate was to be among them. That is where the vision took hold.
She spoke of lobbying efforts to Carson City in 2005 and 2007 for funding – noting funding could only be secured every two years. The first WPI fundraiser was organized in 2005, this coming year they’ll hold their 7th annual. And finally the Whittemore family themselves made a financial commitment. Through this three pronged approach the Whittemore Peterson Institute, in concept and bricks and mortar, was in fact a reality.
She talked about how in early days, when naming the WPI as well as discussing the issue in fundraising, she had to “lose CFS.” She remembered to back when she used the term CFS, it caused more confusion and doubt. This was where the name Whittemore Peterson Institute for Neuro-Immune Disease was born.
Taking it a step further she, along with her WPI cohorts thought, “how could 20 different viruses cause this one disease?” There “must be one underlying cause.” In the research she had performed, simply trying to help her daughter, she saw the glaring similarities amongst CFS, Fibromyalgia, Gulf War Syndrome, Autism, Multiple Sclerosis, Parkinsons. These neuro-immune dysfuctions were common in families and in geographical cohorts. They knew they had something very important on their hands, and they’ve been committed to the neuro-immune cause ever since.
 XMRV – Enter the detection of a brand new retrovirus, XMRV.
XMRV – Enter the detection of a brand new retrovirus, XMRV.
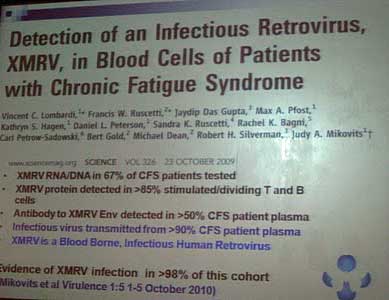
As most of you know, the detection of XMRV in blood cells of patients with CFS was first published in Science, October of 2009. At the time XMRV RNA/DNA was detected in 67% of patients with CFS, XMRV protein was detected in greater than 85% stimulated/dividing T and B cells, and an antibody to XMRV Envelope was detected in over 50% of CFS patients. Exactly one year later Mikovits was published again, after improving on original testing techniques to find XMRV infection in 98% of the original cohort.
And then… there were critics. Some suggested false positives due to mouse DNA contaminations. Others suggested it wasn’t replicable, and therefore claiming false positives.
Both Whittemore and Mikovits addressed the skeptics – confidently, calmly and articulately. Whittemore put it best when sharing what Mikovits has many times reminded her, “positive papers take forever – months or even years to publish. Negative papers only take a few weeks (to publish).”
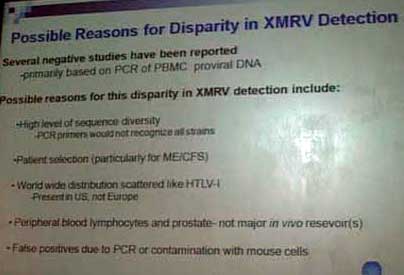 Disparate Results – Reasons for disparity in published results include a high level of sequence diversity in XMRV. A simple PCR would not recognized all the strains. And unfortunately many labs performing the research are not running the exhaustive 5 different tests to confirm XMRV. They have been found to be only running a PCR, which is not exhaustive enough of a test.
Disparate Results – Reasons for disparity in published results include a high level of sequence diversity in XMRV. A simple PCR would not recognized all the strains. And unfortunately many labs performing the research are not running the exhaustive 5 different tests to confirm XMRV. They have been found to be only running a PCR, which is not exhaustive enough of a test.
Whittemore quotes Mikovits here again as saying “Not one virus has ever been discovered through PCR,” basically communicating the frustration – why would they think they could easily find a brand new retrovirus this way all of a sudden? This is why the WPI performs a full 45 day culture on each sample. Mikovits also points out that these exhaustive tests must be run as XMRV lifecycles are not known yet. It may show up under different testing scenarios, depending on the stage of lifecycle it’s in.
Another reason for disparity is related to cohorts. Depending on the criteria used for CFS, the cohorts could include patients who do not in fact have CFS. As we all know, the weaker criteria let patients who suffer from issues such as severe depression fall into the CFS cohort.
Another area that must be considered is the likelihood of disparity in the global distribution of CFS and XMRV. Just as there is in HTLV-1, XMRV will most likely be more prevalent in some countries than others.
Mouse cell contamination causing false positives is absolutely a possibility for disparity. However, when this concern has been raised, the argument has never been able to confirm why CFS patients’ blood comes up XMRV+(leading skeptics to cry contamination) while the “healthy” cohort still not result in high positives. If in fact, there was mouse contamination, both the CFS as well as the healthy cohort would have similar high results of XMRV positive.
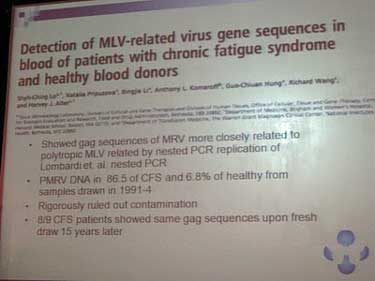 Alter/Lo – Even with skeptics galore, hope is not lost. Enter a second study, confirming what Lumbardi, Ruscetti, Mikovits, et all proposed in Science, October 2009. This paper, known as the Lo/Alter for Dr. Shyh Ching Lo and Dr. Harvey J. Alter, found MRV, closely related to Polytropic MLV, in 86.5% of CFS patients and 6.8% of healthy controls.
Alter/Lo – Even with skeptics galore, hope is not lost. Enter a second study, confirming what Lumbardi, Ruscetti, Mikovits, et all proposed in Science, October 2009. This paper, known as the Lo/Alter for Dr. Shyh Ching Lo and Dr. Harvey J. Alter, found MRV, closely related to Polytropic MLV, in 86.5% of CFS patients and 6.8% of healthy controls.
Again, understanding the nay-sayers to the Science publication, the Lo/Alter team rigorously ruled out contamination. They are the only other study, like that published in Science 2009, that controlled its own samples. If samples are not pristinely maintained (i.e. some might be frozen and thawed repeatedly), “the results will be negative,” confirmed Mikovits.
They took their testing a step further than had been done before. All samples used for this research were from a cohort of CFS patients from the east coast, some 15 years ago. The team tracked down 9 of the patients who were MRV positive and retested them today. All 9 were still positive.
Phylogenetics – The question is always raised – what does MLV or MRV have anything to do with XMRV? Here is a picture of the Phylogenetic Tree of XMRV(P) and Other Gammaretroviruses (updated 1/20/2111). Mikovits mentioned since her original study published in 2009,  she has taken 100 of the CFS samples and retested them with more sensitive testing. 30 of the original 100 have two known sequences, not simply one. The only way to find these is through extensive testing and cultures. Again, why a simple PCR run by these non-successful XMRV replication studies aren’t practicing thorough science.
she has taken 100 of the CFS samples and retested them with more sensitive testing. 30 of the original 100 have two known sequences, not simply one. The only way to find these is through extensive testing and cultures. Again, why a simple PCR run by these non-successful XMRV replication studies aren’t practicing thorough science.
Family Study – Another study, unpublished, but shared with the WPI is from the Cheney Clinic in North Carolina. He tested a group of 47 patients, all families, with 81% positive for XMRV. The findings in this group are astounding. The ratio of male to female was identical. This is NOT a woman’s disease! Half of all family members with a CFS case are XMRV+. And then the list goes on and on of parent/child correlations with CFS, XMRV and Autism.
The WPI followed suit in their own exercise, performing a family study with multiple Neuroimmune Diseases.
In each of the 6 clusters, the top 2 are the parents with the children underneath them. LIGHT BLUE = FIBROMYALGIA, DARK BLUE = CFS, GREEN = AUTISM. Under each shape is their XMRV result. V= virus found in culture, Av = antibody test, NT=not tested
Family 1, upper left corner – One parent XMRV + for virus by culture and XMRV + for antibody, one parent XMRV + for the antibody. Neither parent symptomatic. Child with Autism, XMRV + for the virus.
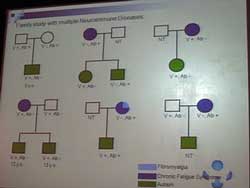 Family 2, top row, middle – One parent with CFS and XMRV+ for antibody. Two children with Autism; one XMRV+ for virus by culture, one XMRV+ by antibody.
Family 2, top row, middle – One parent with CFS and XMRV+ for antibody. Two children with Autism; one XMRV+ for virus by culture, one XMRV+ by antibody.
Family 3, upper right corner – One parent with CFS and XMRV+ for virus by culture. Child with Autism, XMRV+ for virus by culture.
Family 4, bottom left corner – One parent with CFS and XMRV + for virus by culture. Two children with Autism, both XMRV+ for virus by culture.
Family 5, bottom row, middle – One parent with CFS, Fibromyalgia and XMRV+ by antivody. Child with Autism, XMRV+ for virus by culture and by antibody.
Family 6, bottom right corner – One parent with CFS and XMRV+ by antibody. Child with Autism, not tested for XMRV.
A quick summary provided by Dr. Mikovits regarding families. She can confirm, there is XMRV in children under the age of 5. To date they have confirmed XMRV in 16 of 17 families with neuroimmune disease amongst multiple members. Finally, that more work needs to be done to confirm pathogenesis and transmission.